Digestion and Absorption
Vitamin C does not require digestion prior to being absorbed into intestinal cells. Ascorbic acid is absorbed in the body by both active transport and simple diffusion. Absorption using active transport includes sodium-dependent cotransporters (two SVCTs: SVCT1 & SVCT2) and hexose transporters (GLUT1 & GLUT3). SVCTs are responsible for the uptake of vitamin C in most organs. SVCT1 is typically found in epithelial tissue while SVCT2 is found in most tissue (especially the brain) except the lungs and skeletal muscles.
Both transporters import the oxidized form of ascorbic acid across the basolateral membrane of the intestinal cells. GLUT1 and GLUT3 transfer only the dehydroascorbic acid (DHAA) form of vitamin C. DHAA is usually absorbed more rapidly than ascorbate; however, small amounts are found in tissues due to cells converting DHAA back to ascorbate. Therefore, SVCTs are the primary system for transporting vitamin C throughout the body. Simple diffusion typically occurs in the mouth and stomach. When higher amounts of vitamin C are consumed, simple diffusion is used for absorption.
Vitamin C does not require digestion prior to being absorbed into intestinal cells. Ascorbic acid is absorbed in the body by both active transport and simple diffusion. Absorption using active transport includes sodium-dependent cotransporters (two SVCTs: SVCT1 & SVCT2) and hexose transporters (GLUT1 & GLUT3). SVCTs are responsible for the uptake of vitamin C in most organs. SVCT1 is typically found in epithelial tissue while SVCT2 is found in most tissue (especially the brain) except the lungs and skeletal muscles.
Both transporters import the oxidized form of ascorbic acid across the basolateral membrane of the intestinal cells. GLUT1 and GLUT3 transfer only the dehydroascorbic acid (DHAA) form of vitamin C. DHAA is usually absorbed more rapidly than ascorbate; however, small amounts are found in tissues due to cells converting DHAA back to ascorbate. Therefore, SVCTs are the primary system for transporting vitamin C throughout the body. Simple diffusion typically occurs in the mouth and stomach. When higher amounts of vitamin C are consumed, simple diffusion is used for absorption.
The degree of vitamin C absorption decreases as intake of this vitamin increases. A normal intake of vitamin C has an absorption rate ranging from 70% to 95% (30-180 mg/day). So, consuming1.5g of ascorbic acid results in 50% absorption while ingesting over 12g causes only 16% of the vitamin to be absorbed. An intake of < 20mg has an absorption rate of 98%. Vitamin C absorption is greater when individual doses, <1g, are consumed throughout the day rather than in one mega-dose. Absorption can be reduced when there is a high amount of intracellular glucose (interferes with ascorbate transporters).
Once ascorbate enters intestinal cells, it diffuses through anion channels in its free form (an ascorbate anion) into extracellular fluid and enters the plasma by capillaries. Absorbed ascorbic acid and DHAA can either be transported freely or bound to albumin. Ascorbate can also move into body cells and tissues. The adrenal and pituitary glands, red blood cells, lymphocytes, and neutrophils all receive vitamin C in the form of DHAA. Intestinal flora metabolizes any unabsorbed vitamin C. Consuming high amounts of iron containing vitamin C can cause oxidative destruction of this vitamin in the digestive tract (produces diketogulonic acid) impair uptake. Mega-dosing of vitamin C can saturate the enzyme kinetics of this vitamin. This leads to excess ascorbic acid in the intestinal lumen which causes various gastrointestinal problems. Zinc and pectin has also shown to inhibit ascorbic acid as well.
Once ascorbate enters intestinal cells, it diffuses through anion channels in its free form (an ascorbate anion) into extracellular fluid and enters the plasma by capillaries. Absorbed ascorbic acid and DHAA can either be transported freely or bound to albumin. Ascorbate can also move into body cells and tissues. The adrenal and pituitary glands, red blood cells, lymphocytes, and neutrophils all receive vitamin C in the form of DHAA. Intestinal flora metabolizes any unabsorbed vitamin C. Consuming high amounts of iron containing vitamin C can cause oxidative destruction of this vitamin in the digestive tract (produces diketogulonic acid) impair uptake. Mega-dosing of vitamin C can saturate the enzyme kinetics of this vitamin. This leads to excess ascorbic acid in the intestinal lumen which causes various gastrointestinal problems. Zinc and pectin has also shown to inhibit ascorbic acid as well.

Storage and Excretion
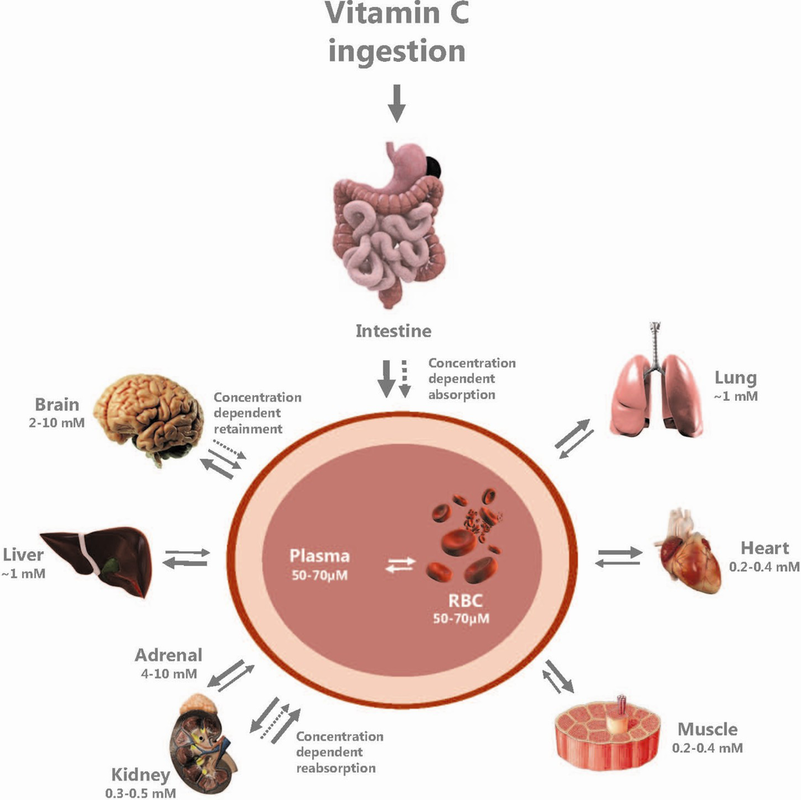
Vitamin C is stored throughout the body’s tissues and blood. The pituitary glands, adrenal glands, and the eye lens contain the highest vitamin C content. On the contrary, the saliva and plasma have the lowest ascorbate content. Tissue concentrations exceed those found in the plasma by three to ten times. Active transport pumps are responsible for the higher tissue concentrations of vitamin C versus the plasma. Only small amounts of dehydroascorbate appear in the blood, because of rapid cellular uptake by GLUT transporters.
Abscorbic acid has a half-life of 16-20 days and is excreted in the urine. Metabolites of vitamin C including DHAA, oxalic acid, 2-O-methyl ascorbate, and 2-ketoascorbitol are also excreted from the body by urine. DHAA and ascorbic acid can be reabsorbed in the kidney tubules when body pool levels are equal or less than 1500mg. The excretion of vitamin C in the urine does not occur when levels are lower than 1500mg. Levels higher than 1500mg cause the reabsorption efficiency of the kidneys to decrease. Body pool levels from 1500-3000mg relate to tissue saturation of this vitamin. Plasma ascorbate levels between 0.8-1.4mg/dl are considered the renal threshold. Vitamin C will be excreted rather than reabsorbed when above these levels.
Vitamin C is stored throughout the body’s tissues and blood. The pituitary glands, adrenal glands, and the eye lens contain the highest vitamin C content. On the contrary, the saliva and plasma have the lowest ascorbate content. Tissue concentrations exceed those found in the plasma by three to ten times. Active transport pumps are responsible for the higher tissue concentrations of vitamin C versus the plasma. Only small amounts of dehydroascorbate appear in the blood, because of rapid cellular uptake by GLUT transporters.
Abscorbic acid has a half-life of 16-20 days and is excreted in the urine. Metabolites of vitamin C including DHAA, oxalic acid, 2-O-methyl ascorbate, and 2-ketoascorbitol are also excreted from the body by urine. DHAA and ascorbic acid can be reabsorbed in the kidney tubules when body pool levels are equal or less than 1500mg. The excretion of vitamin C in the urine does not occur when levels are lower than 1500mg. Levels higher than 1500mg cause the reabsorption efficiency of the kidneys to decrease. Body pool levels from 1500-3000mg relate to tissue saturation of this vitamin. Plasma ascorbate levels between 0.8-1.4mg/dl are considered the renal threshold. Vitamin C will be excreted rather than reabsorbed when above these levels.